$AEGR - Aegerion Pharmaceuticals
Aegerion is developing a single drug, lomitapide, for a severe, orphan disease known as homozygous familial hypercholesterolemia (HoFH). Their main rival in this pursuit is Isis Pharma $ISIS and their drug KYNAMRO (mipomersen). Learn more about these drugs and HoFH here. Both drugs have pending New Drug Applications (NDAs) with the FDA, and the PDUFA decision dates are in January 2013.
FDA Advisory Panel
AEGR is in the news because the FDA Endocrinologic and Metabolic Drug Advisory Committee will review the NDA for lomitapide on 10/17/2012, to be followed with discussion of the Isis drug on 10/18/2012. You can find all the information about the AdCom at this link, including:
- Draft agenda for the say
- Draft version of the questions the panel will discuss. There is also a single voting question.
- Roster of the committee members
- Briefing documents prepared by the FDA and by the Sponsor (Aegerion). Note that you only really need to read the FDA version.
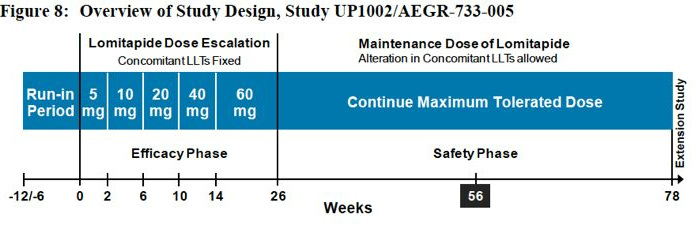
AEGR Lomitapide phase 3 trial design - from sponsor briefing document
FDA Briefing Documents - what have we learned?
Find below some key information and comments from the FDA briefing documents released 10/15/2012. Most of the document is from the clinical reviewer (Medical Officer), but there are also comments from Clinical Pharmacology, Statistics, Pharmacology-Toxicology, and the Risk Evaluation and Mitigation System (REMS) staff. Note we heard nothing about chemistry/manufacturing/controls because this is not a topic of discussion for the committee. Comments/questions in italics are my thoughts, otherwise they reflect the comments of the FDA reviewer in the briefing book.
- 31% of phase 3 patients had less than 15% improvement in LDL (see waterfall plot below)
- FDA estimates HoFH as 1:1 million, or about 300 in US (a much smaller number than the one thrown around by ISIS)
- liver fat seems to go away, but FDA notes they have no idea as to whether there is any histological sequelae because no liver biopsies were performed... and there is "significant concerns of patient harm" from hepatic steatosis - limits use to narrow population at very high risk
- phase 2 proof-of-concept trial had 6 patients (provided supporting efficacy/safety data only. I will spare the comparisons to SRPT regulatory situation if such a trial came along in 2012)
- FDA suggested the single arm study in HoFH with a properly conducted run-in period in order to increase the safety database of HoFH patients vs. a placebo-controlled trial. FDA wanted 36 pts, sponsor lowered to 25 because thought would have difficulty recruiting in US, FDA questioned decision at the time (but did not seem to change conclusions of briefing document author). FDA concurred with dose escalation scheme
- FDA mentions possible drug-induced fat accumulation in intestine and lung as well, but in much less detail.
- 11/2009 end of phase 2 meeting to discuss broader populations- agency raised concerns over carcinogenicity study results. FDA would allow refractory heterozygous FH trial, but AEGR also must do high risk HeFH trial, and may need clinical outcomes trial. AEGR has not pursued any of these options, at least in part due to financial constraints.
- including patients with >300 LDL mimics the severe refractory HeFH population and shifts risk/benefit (untreated HoFH have LDL 650 mg/dL) -this would be a REMS issue
- safety, but not effiacy data for weeks 56 through 78 have been submitted to the NDA
- It seems unclear whether lomitapide would be approved for patients with liver related abnormalities based on clinical pharmacology comments - what portion of the market would this represent?
- 24/28 patients (86%) had >10% increase in % hepatic fat (absolute points, see figure below) - patients with diabetes or alcohol consumption were excluded from study but have greater risk of steatosis. 26% missing data - may be biased and missing subjects with large amounts of fat at follow-up. appears reversible (not always), at least after short term use
- substantial fat accumulation even in the clinical trial with lower risk patients at lower doses of 2.5-10 mg.
- investigators were not blinded to LDL levels - potential bias source
- Pivotal trial: average age 30, avg BMI 25.8 - only one qualified as obese (not the population you picture in your mind for a CV/cholesterol drug). All had documented LDL receptor genetic defects (Isis often says that HoFH is not often genetically diagnosed in practice, seemingly in stark contrast to this trial population...which is more accurate in the real world?). 62% on apheresis, 93% on statins. Mean entry LDL 336 (range 152-564). Fat-soluble nutrients were supplemented in this trial
- those patients (n=23) who made it to 6 months without dropping out stayed on drug for full 78 weeks, and at stable doses
- timing between aphaeresis and LDL measurement had the potential to introxduce bias, but appeared not to
- mean change in HDL and apoAi are "in clinically undesirable direction" at 26 weeks
- "it should not be assumed that reducing freqency or stopping apheresis will benefit pts with HoFH" (this conclusion refutes a claim made in the Sponsor's document) - net risk benefit of apheresis+lomitapide is unknown
- weak evidence that hepatic fat accumulated is associated with high LDL declines, but limited power to see such an effect with 22 patients (Isis claims that there is such a correlation - we will see what their briefing document say tomorrow).
- Statistical reviewer: the trial showed that the drug was successful in reducing LDL-C, total cholesterol, ApoB, triglycerides, non-HDLC, and V-LDLC after 26 weeks of treatment and maintained through 56 weeks. No efficacy difference between 40 and 60 mg doses. LpA reduced only at 56 weeks not 26.
- "It is unknown if long-term exposure to lomitapide will cause irreversible liver injury. The potential for progression of non-alcoholic fatty liver (NAFL) to non-alcoholic steatohepatitis (NASH) is unknown, but should this occur, the potential consequences could be severe. Patients would be at risk for cirrhosis and liver-related death. Because of the severity of vascular disease in patients with HoFH, they may benefit from treatment with lomitapide, even though the liver safety issue has not been fully characterized."
- If approved, must have safeguard so only access for patients with proper risk/benefit . But will not require genetic diagnosis of HoFH. (this was not well defined, and may be a topic of discussion by the panel - and will play a role in determining commercial opportunity)
- Goals: educate prescribers, limit access. Certify prescribers and pharmacies, give Medication Guide to patient. No enrollment or specific patient monitoring will be required.
Individual Patient Data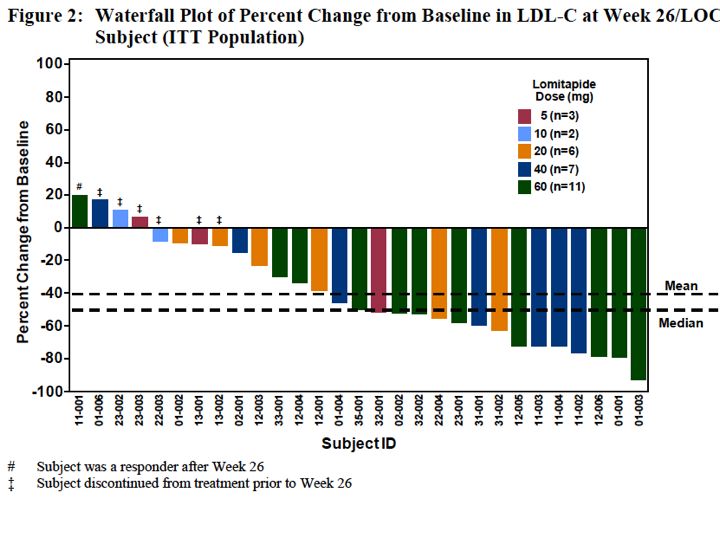
AEGR lomitapide HoFH phase 3 trial - individual patient LDL change waterfall plot. From sponsor briefing document
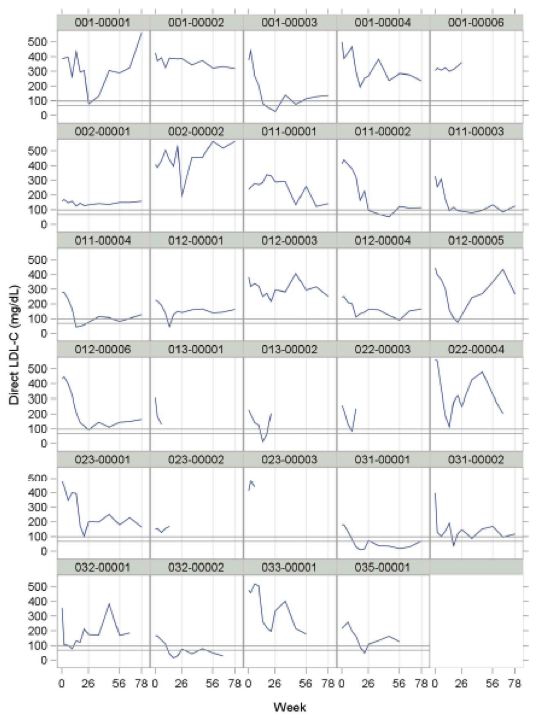
individual patient LDL levels - lomitapide phase 3 trial
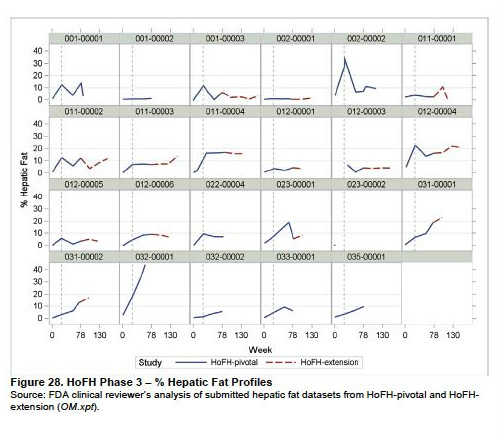
individual patient liver fat - lomitapide phase 3 trial
|
|
