- My notes from the Synta webcast at the Lazard conference on 11/15 are below
- For company info featuring ganestespib HSP90 inhibitor can see SNTA research page
- For complete event calendar and links to my notes see Upcoming Events page.
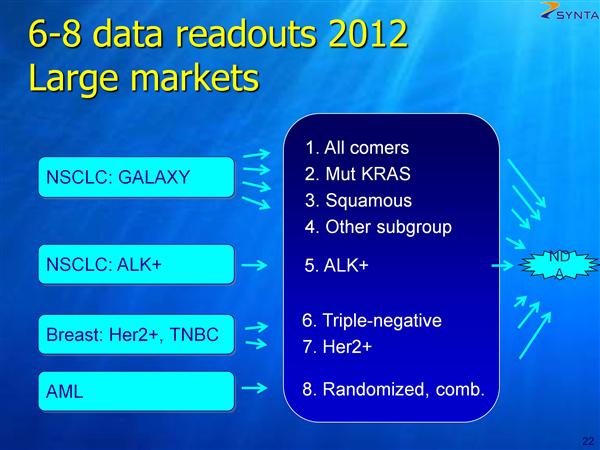
- 6-8 readouts in next 12 months for ganetespib, each potentially leading to NDA path (more details in figure below) including the following:
- ALK+ NSCLC - terrific single agent data, similar to early crizotinib data
- Striking data in breast cancer, global program initiating now
- AML 1st line randomized trial - run by cooperative group
- Breast cancer previous trial of 17-AAG added to Herceptin saw tumors shrinkage in 2/3 of patients
- New patient scan slide - 12 month crizotinib partial repsonse then failure. Saw significant response after 3 doses of ganetespib - helps show that the two drugs work via different mechanisms in the same patient population.
- Very nearly everyone we talk to in the lung cancer field wants to give Xalkori (crizotinib) and ganetespib together - and that IS what the future of this treatment is going to be
- Recap of ALK+ data presented this year: 4/8 patients had PR (durable at least 10 months) with single agent ganetespib. Pfizer went to the FDA with just 7 responses!
- INFI drug showed response in 2/3 ALK+ patients, so total for the two HSP90 inhibitors is 6/11. [It is interesting to note that since this data release, INFI has made not even a peep about pursuing the ALK population with their drug IPI-504, a first generation HSP90 inhibitor that previously failed in GIST due to severe side effect issues. The lung cancer community is clearly not interested either. Also, INFI clearly believes that HSP90 inhibitors - or at least theirs I guess - will not work as single agents and must be combo trials. SNTA clearly disagrees with this, at least for carefully chosen patient subpopulations]
- 50,000 patients per year have lung cancers understood to be driven by EML4-ALK fusion protein. Hope to convert from fatal to chronic condition, causing a shift from treating prevalence instead of incidence. This transition is what helped make Herceptin and Gleevec multi-billion dollar drugs. That's why i think Crizotinib will be very successful - and we're very fortunate to be the second drug after them
- 3 company sponsored legs of the ganetespib "stool"
- 240 patient phase 2b (much larger than typical 80-100 patients) - gives us an opportunity to enrich the phase 3 population - and represents four of the 2012 shots on goal mentioned above. [the info below is BY FAR the most clarity SNTA has ever given around the details of this trial]
- >90% powered to see a 3-4.5 month PFS improvement in the full intent-to-treat (ITT) population - this is first co-primary endpoint
- 2nd co-primary endpoint is the k-Ras mutant subpopulation - also 90% powered to see ~100% improvement - because progression is so fast on this arm
- Squamous cell histology sub population
- undisclosed proprietary biomarker
- Trial has 60 sites, majority in the EU, trial will be completely enrolled in ~ April
- Interim data will be available in about the April timeframe as well, PFS data 3q2012, OS data by year-end 2012
- We're in discussions now on how to design this to be a registration-enabling program
- It's going to be more than one trial
- Development like Tykerb - which was evaluated after, with, and before Herceptin
- Triple negative (TN) - does not express estrogen receptor (ER), progesterone receptor (PR, or Her2/neu genes
- Her2 positive
Partnering and Cash
- Q42011/1H2012 - on track for one or more deals [another slight slip in the timeline for this guidance]
- Most advanced discussions center around Asian rights to HSP90 program/ganetespib - this is "most likely by early in the new year"
- preclinical CRACM program also under discussion
- Cash on hand is sufficient well into 2012 - plus additional money from partnership that we're in pretty advanced discussions on now [a big Asian deal simply has to come or Synta cannot come close to paying for the ganestespib trials outlined above. The company has already - wisely in my opinion - scrapped plans to run more company sponsored trials of elesclomol at this time]
Question and Answer Session:
Will you move directly into phase 3 for the Her2 and triple negative breast cancer indications?
For breast cancer we would do phase 2 first. For the GALAXY trial and for the ALK+ NSCLC indication, moving directly into registrational studies.
Will you move directly into phase 3 for the Her2 and triple negative breast cancer indications?
For breast cancer we would do phase 2 first. For the GALAXY trial and for the ALK+ NSCLC indication, moving directly into registrational studies.
 RSS Feed
RSS Feed
